
The DEA currently categorizes marijuana as a Schedule I drug, including it with a group of other dangerous drugs that have “no currently accepted medical use.” Therefore, most people are rightly surprised when they learn that the U.S. government, through the Department of Health and Human Services, holds a patent on the use of cannabinoids for a variety of potential medical applications. In its patent filing the government states:
“Cannabinoids have been found to have antioxidant properties…This new found property makes cannabinoids useful in the treatment and prophylaxis of wide variety of oxidation associated diseases, such as ischemic, age-related, inflammatory and autoimmune diseases. The cannabinoids are found to have particular application as neuroprotectants, for example in limiting neurological damage following ischemic insults, such as stroke and trauma, or in the treatment of neurodegenerative diseases, such as Alzheimer’s disease, Parkinson’s disease and HIV dementia.”
Now take a deep breath, and let’s take a look at how cannabinoids function to make the cannabis plant such an effective medical remedy.
How do Cannabinoids Work?
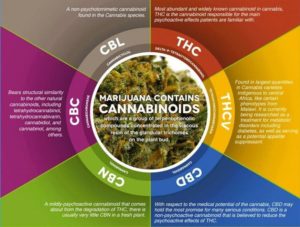
Cannabinoids are the chemical compounds secreted in cannabis flowers. There are more than 100 confirmed cannabinoids. Although some cannabinoids exist in other plants, the vast majority are found only in cannabis.
Cannabinoids work by attaching to specific receptors, called endocannabinoid receptors, which are found all over the human body. The endocannabinoid system is responsible for regulating a broad range of important biological functions including appetite, sleep, emotional behavior, body temperature and movement.
There are two primary endocannabinoid receptors – CB1 and CB2. CB1 receptors work primarily on the brain and are predominantly located in the central and peripheral nervous systems. CB2 receptors, on the other hand, work mainly on the body and are found mostly in the immune system. When cannabis is consumed, cannabinoids bind to these receptor sites. When a particular cannabinoid or combination of cannabinoids attach to these specific receptors, it triggers a series of changes in the way cells send signals to other cells throughout the body.
Each cannabinoid produces different physical and psychological effects based on the particular receptors that they bind to. Delta-9-THC, more simply known as THC, is the most abundant cannabinoid in the cannabis plant. It is also the cannabinoid that demonstrates the highest level of psychoactivity (i.e. it’s responsible for the “high” that users feel when they consume marijuana). While THC shows a robust affinity for CB1 receptors in the brain, lesser known cannabinoids such as CBN (cannabinol) are known to bind to CB2 receptors in the body. By targeting the right cannabinoid at the right receptor, it is possible to achieve different results.
The Endocannabinoid System
The body produces its own endogenous cannabinoids, the most prominent of which is anandamide. Anandamide is the chemical responsible for activating cannabinoid receptors. THC is the phytocannabinoid counterpart to anandamide. It shares most of the same pharmacological properties and mimics its actions. On its own, the anandamide level in the body is very low and is quickly broken down by an enzyme known as fatty acid amide hydroxylase, or FAAH. When anandamide interacts directly with external cannabinoids such as THC or CBD we see very different results.
To truly grasp how the endocannabinoid system works, it’s important to first understand how brain cells communicate with each other and the rest of the body.
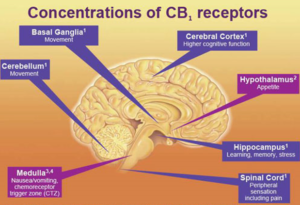
Location of CB1 receptors in the brain
The brain has hundreds of billions of nerve cells called neurons. These are the cells that send the signals to and from the brain and to the other parts of the body. The neuron is comprised of a cell body, and from that cell body are tiny branches called dendrites which act as receivers for the neuron. The cell body also has a long projection called the axon, and at its end are axon terminals which serve as the transmitters of the neuron.
Now, imagine that all these neurons are connected, but in between the axon terminals and the dendrites are gaps called the synapse. The presynaptic cell (the transmitter neuron) releases chemicals (neurotransmitters) that travel across the synapse to the postsynaptic cell (receiver neuron) “passing the message” until it reaches the specific part of the brain that reacts to that particular chemical.
The endocannabinoid system works differently. Essentially, it acts in reverse order. Once the postsynaptic cell is triggered, endogenous cannabinoids are released by the neuron’s endocannabinoid system. The endogenous cannabinoids then travel back to the presynaptic cell and attach to its cannabinoid receptors. Because cannabinoids primarily affect the presynaptic neuron, they can control how the signals are received, relayed, interpreted, and transmitted back to the rest of the neurons. Once the cannabinoids enter the body, they immediately begin to interfere with the actions of the endogenous cannabinoids. Think of these cannabinoids as something that “softens” the effects of how the signals are received, interpreted, and sent back to the body.
Cannabinoid Therapy
To quickly recap, there are many different types of cannabinoids, and they each have different effects on the body based on the particular endocannabinoid receptors with which they interact. Because endocannabinoid receptors are found all over the body, the potential therapeutic benefits from the plant’s cannabinoids are widespread.
For example, we know that cannabinoids can be extremely useful in helping to control seizures. One cannabinoid in particular, cannabidiol (CBD), has been the focus of quite a bit of news coverage recently, leading many to believe that CBD oil alone can serve as a panacea for people living with epilepsy. CBD is non-psychoactive, so it’s understandable why taking this route of treatment is a preferred option when compared to a whole plant extract containing psychoactive THC. However, while CBD is a vital component of a cannabinoid-based therapy for epilepsy, most patients don’t get relief from CBD oil alone. Here’s why:
One of the critical functions of the CB1 receptor is the regulation of excessive or inadequate signaling by the neurotransmitters in the brain. Glutamate is the primary neurotransmitter that triggers and increases the excitability of neurons. It is also the principal neurotransmitter that facilitates the spread of seizure activity. By activating the CB1 receptor, we can inhibit the release of glutamate, thus regulating the neurotransmitter back into balance.
THC has a strong affinity for the CB1 receptor. Anandamide, the body’s endogenous cannabinoid, also favors the CB1 receptor. CBD, on the other hand, has a minimal binding affinity for the CB1 cannabinoid receptor. Instead, CBD indirectly stimulates endogenous cannabinoid signaling by suppressing FAAH. As mentioned above, FAAH is the enzyme involved in the metabolic breakdown of anandamide. With FAAH contained, it means that higher levels of anandamide remain in the body for a longer duration. Greater levels of anandamide result in greater CB1 activation.
So let’s break it down. THC, in conjunction with anandamide, activates the CB1 receptor. This activation brings the neurotransmitters back into balance, resulting in decreased seizure activity. CBD inhibits the enzyme that metabolizes and degrades anandamide, improving the results by enhancing the body’s innate protective endocannabinoid response. Notably, CBD also opposes the action of THC on the CB1 receptor, thereby lessening the psychoactive effects of THC. This synergistic effect of multiple cannabinoids working in concert is known as the entourage effect.
The Entourage Effect
The concept of the entourage effect was coined by Israeli scientists Shimon Ben-Shabat and Dr. Raphael Mechoulam (the Father of Cannabis research). In a nutshell, the entourage effect just means that for cannabis to work most effectively as a medical treatment, there should be a harmonious interaction of the different types of cannabinoids. This discovery has significantly affected the way scientists look at the plant. By breeding cannabis strains that contain greater levels of specific cannabinoids, scientists believe they can formulate better medications to treat a variety of conditions with lower risks of adverse side effects.
There has been a substantial amount of research conducted on the effects of THC and CBD in isolation. THC has been shown to have anti-inflammatory, analgesic (pain relief) and antiemetic (prevents vomiting) properties. CBD has been demonstrated to possess anti-anxiety, anti-psychotic, and anti-seizure attributes. However, mounting evidence has shown that isolating these cannabinoids, or creating them in a lab (synthetic cannabinoids), may limit their therapeutic use.
Take a look at Marinol, an FDA-approved drug that contains synthetic THC and is often prescribed to patients who are undergoing chemotherapy. While it purportedly offers the same effects of the real cannabis plant by reducing the side effects of chemotherapy, it also creates a host of adverse side effects. Users often experience confusion, mood changes, irritability, depression, memory problems, etc. – likely because the drug does not contain CBD, which is known to counteract some of the effects of THC.
Lesser Known Cannabinoids
We have touched on the two primary cannabinoids, THC and CBD. There are also some lesser known cannabinoids that research has demonstrated to have substantial potential therapeutic value.
- CBC (Cannabichromene): After THC and CBD, CBC is the third most common cannabinoid. Similarly to CBD, CBC is non-psychoactive. Research suggests that CBC has, to varying degrees, anti-inflammatory, anti-tumor, anti-depressant and anti-fungal properties. The therapeutic value of CBC is significantly improved when combined with other cannabinoids such as THC, CBD, and CBG. CBC has also been shown to promote the growth of new brain cells (neurogenesis), which indicates the possibility of its efficacy a preventative treatment for conditions such as Alzheimer’s Disease.
- CBN (Cannabinol): CBN is a cannabinoid that is produced when THC breaks down – most commonly when cannabis flowers grow old and stale. Therefore it’s not surprising that CBN has mild psychoactive properties. CBN has been shown to substantially increase appetite (even more than THC) as well as function as an antibiotic and anti-inflammatory. It has powerful sedative and pain relieving qualities. It has also been shown to lessen ocular pressure which makes it of potential therapeutic value for glaucoma patients. Most interestingly, a 2005 study on mice with a rodent version of Lou Gehrig’s disease found that CBN delayed on the onset of symptoms. These findings signal the potential for CBN to ease the symptoms of patients with progressive neurodegenerative diseases such as ALS.
- CBG (Cannabigerol): This cannabinoid is typically found only in minute quantities because it is only present during the early growth cycle of the cannabis plant. It is non-psychoactive, and thus a prime target for medical research. Studies have demonstrated this cannabinoid to have antibiotic, antifungal, and anti-depressant properties. It has shown the potential to promote bone growth and treat skin diseases such as psoriasis. It has also been proven to have mild anti-tumor effects for certain types of cancer and is believed to be a more powerful painkiller than THC.
- THCV (Tetrahydrocannabivarin): THCV is a mildly psychoactive cannabinoid that is only found in some strains of cannabis and typically in small concentrations. While it is structurally very similar to THC (the only difference is that the THCV molecule has three carbons while the THC molecule has five carbons), the effects that each cannabinoid produce are very different. While THC is known to stimulate appetite, THCV suppresses appetite. THCV also counteracts some of the negative, anxiety-related psychoactive effects of THC. Additionally, research has shown that THCV has antiepileptic and neuroprotective properties.
- CBDV (Cannabidivarin): CBDV is a slightly degraded version CBD. As with THCV and THC, small changes to the molecule can result in potentially significant variations in the way this cannabinoid interact with the body. There has not been a tremendous amount of research done on CBDV, but the limited studies conducted to date have demonstrated that this cannabinoid has the potential to help epileptic patients and patients with gastrointestinal problems.
- Delta-8-THC: This cannabinoid is a milder form of THC that has fewer psychoactive effects. More research is required, but early studies have shown that Delta-8-THC has powerful appetite-stimulating and anti-nausea properties.
As the overwhelming evidence shows, the potential medical benefits of cannabinoids are almost limitless. We have barely scratched the surface of our knowledge of this incredible plant. With the gradual relaxation of cannabis laws across the country, the next 10 to 20 years are likely to result in a flood of new scientific and medical discoveries.
Leave a Reply
You must be logged in to post a comment.